


This week kicks off Black, Indigenous, persons of color (BIPOC) Mental Health Month. What does your program have planned for this week to raise awareness of mental health disparity? As mental health advocates, we need to create actionable steps to raise awareness and reduce the chasm of care experienced by persons of color. This year’s theme for BIPOC MHM is Culture, Community, & Connection. According to Mental Health America, our lives are deeply intertwined with our environments, and these surroundings impact our mental health and overall wellness. BIPOC populations are faced with disproportionate amounts of historical trauma and displacement that can challenge their ability to thrive in their environments. However, culture, community, and connection are pillars that support and uplift BIPOC individuals in the face of oppression and systemic racism.
Here is the link to the BIPOC MHM toolkit for your use throughout the month.
As we look at the disproportionate effects of mental illness across varying populations the data is staggering. This week we will start with looking at mental health statistics for the African American community.
How Does Mental and Behavioral Health Affect African American Populations?
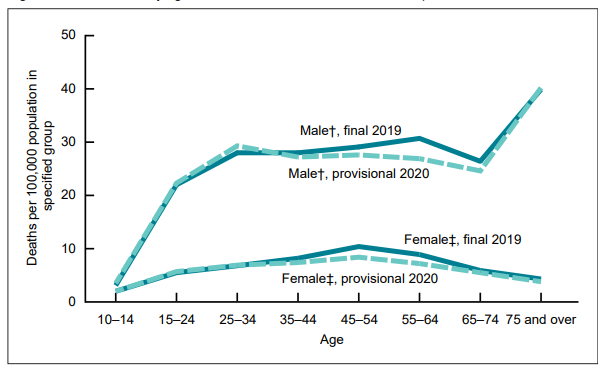
• In 2020, suicide was the third leading cause of death, respectively, for blacks or African Americans, ages 15 to 24.1
• The death rate from suicide for black or African American men was four times greater than for African American women, in 2018.
• The overall suicide rate for black or African Americans was 60 percent lower than that of the non-Hispanic white population, in 2018.
• Black females, grades 9-12, were 60 percent more likely to attempt suicide in 2019, as compared to non-Hispanic white females of the same age.
• Poverty level affects mental health status. Black or African Americans living below the poverty level, as compared to those over twice the poverty level, are twice as likely to report serious psychological distress.
• A report from the U.S. Surgeon General found that from 1980 – 1995, the suicide rate among African Americans ages 10 to 14 increased 233 percentage, as compared to 120 percent of non-Hispanic whites.
In the coming weeks I am going to share about behavioral health equity and actions we can take to work toward a world where all individuals, regardless of race, age, ethnicity, gender, disability, socioeconomic status, sexual orientation, or geographical location, has access to high-quality and affordable healthcare services and support.









{kind=link}
{kind=link}
{kind=link}